

Servikal İntraepitelial Neoplazi Nedir? Nasıl Tedavi Edilip İzlenir? (SIN / CIN ya da LSIL /HSIL)
Aslında kafanızın karışması normal bizimki de çok karışmadı zamanında 🙂 🙂
Dolayısıyla kitaplarda “Terminoloji” başlığında anlatılan konuya hoş geldiniz.
Eskiden beridir rahim ağzının kanser öncülü (prekanseröz) lezyonlarını “Displazi” olarak adlandırıyoruz. Displaziler aslında “Servikal İntraepitelial Neoplazi” olarak tanımladığımız lezyonlar.
Yani nedir efendim:
“Servikal” yani rahim ağzında yer alan, “intraepitelial” yani epitel dediğimiz (ki cildimizi de benzer bir doku) dokunun içinde yer alan dışına taşmayan, “bazal membran” dediğimiz alt katmanı geçmeyen, “neoplazi” yani anormal gelişmiş dokulardır displaziler.
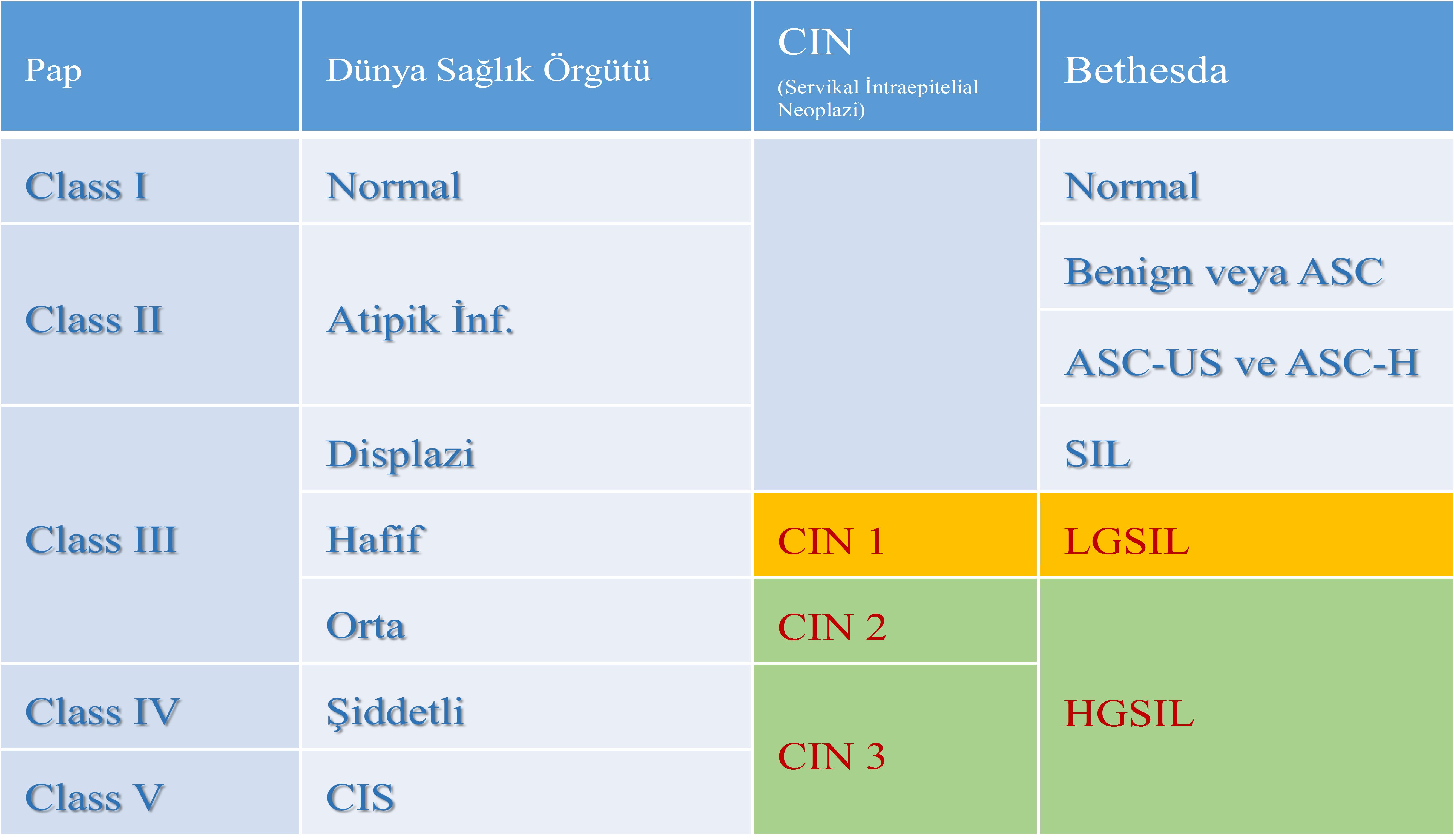
Displazileri de kendi içinde 3’e ayırıyorduk: Hafif (CIN I) Orta (CIN II) ve Ağır (CIN III)
Daha sonra 1988 yılında Amerikalılar biraz da literatürü kendileri domine etmek istedikleri için Bethesta sistemini getirdiler. Bu sınıflama çok mükemmel (!) olduğu için 1991 ve 2001 yıllarında 2 kez revize edildi.
Bu sistemede sitolojik hücrelerde (Smear de elde edilen hücrelerde) ve histolojik değerlendirmede (kolposkopi altında yapılan biyopsilerde) elde edilen hücrelerde farklı adlandırma yapıldı:
Pap smearde elde edilenler anormal hücreler için “Skuamöz intraepitelial neoplazi”, alınan biyopsilerden elde edilen hücreler için ise “servikal intraepitelial neoplazi” tanımlaması (Şu meşhur CIN olayı) kullanıldı.
Eee bana ne bu detaylardar derseniz. Sizi ilgilendiriyor zira elinize aldığınız patoloji raporunda mors alfabesi gibi yazılmış onlarca büyük harf kodlaması görüp sonra da “Google ana”nın kucağına atlıyorsunuz.
Okuduğunuz ve çoğunu anlamadığınız ki biz de bazılarını anlamıyoruz, tanımlamalardan sonuç çıkarmaya çalışırken sonunda “Evet ya kesin kanser oldum” noktasına varıp mebzul miktarda meslektaşımın ve benim telefonumu çaldırıyorsunuz.
İnanın çaldırmanız sorun değil de, bunca detayı telefonda açıklamaya çalışmak ama en önemlisi “kanser” olmadığınızı anlatmak çok zor oluyor. Dolayısıyla önemli 🙂 dostlarım. Ben anlatmaya, siz okumaya devam.
CIN’lerde kalmıştık. O zaman “Servikal İntraepitelial Neoplazi” (Cervical Intraepithelian Neoplasia) ne demek hücresel bağlamda dilimiz döndüğünce anlatalım:
Rahim ağzının dış kısmı, muayenede görülen kısmı skuamöz epitel ile kaplıdır. İşte bu dokunun en alt tabakası “bazal tabaka” diğer bir değiş ile temel tabakadır. Anormal hücreler, displazik hücreler, bazal tabakayı geçmedikleri sürece kanserden bahsedemeyiz! Bunu anlamanız önemli.
İşte bazal tabakanın üstünde kalan alanı patologlar kabaca üçe bölüyorlar.
CIN I: Bazal tabakanın üzerinde ki skuamöz epitel dokunun en alt, bazal tabakaya komşu 1/3’lük kısmında anormal, displazik hücrelerin bulunması durumudur.
CIN II’de ise skuamöz epitelin alt kısmından itibaren 2/3 kısmında displazik hücrelerin bulunmasıdır.
CIN III’de ise anlayacağınız gibi tüm epitelial katmanlarda anormal hücreler mevcuttur.
Bu noktada “Karsinoma in situ” tanımının üzerinde durmak gerek. Açıkçası “Karsinoma in situ” ile CIN III ya da HSIL arasında ki fark patologların arasında devamlı tartışılır.
Ve ne yalan söyleyeyim klinik bağlamda benim hastaya uygulayacağım tedaviyi değiştirmez. Ama klasik ekole bağlı ve sadece bu konu ile iştigal eden patologlar açısından “Karsinoma in situ” tanısı önemlidir ve ayırım mutlaka yapılmalıdır.
Örneğin değerli dostum patolog Prof.Dr.Ekrem Yavuz’un bu konuyu tartışırken “Ben kadın olsam karinoma in situ olup olmadığımı bilmek isterdim” dediğini gayet iyi hatırlıyorum.
Diğer taraftan şu terminoloji olayı da bitmek bilmedi.
2001 yılında Bethesta sistemi yenilendikten sonra bu sefer de 2012 yılında “Lower Anogenital Squamous Terminology (LAST)” projesi kapsamında CIN I’lere “Low Grade Squamous Intraepithelial Lesion = LSIL” denilmesine, CIN II ve III lezyonların ise “High Grade Squamous Intraepithelial Lesion = HSIL” olarak adlandırılmalarına karar verildi.
Ya yeter artık ne uğraşıyorlar derseniz valla ben de bilmiyorum ama konuştuğum yurdum topraklarında ki patoloji hocalarının anlattıkları onlarca öykü var.
Ama konu ile ilgili, benimde şahit olduğum en ilginç olaylardan biri 2010 yılında sadece HPV konuşulan “Eurogyn” toplantılarının birinde Fransız bir patolog meslektaşımızın kürsüye çıkıp “Yeter ben CIN II’mi geri istiyorum, size yedirmem” demesidir. O derece yani 🙂
(Not: Fransız profesör harbiden böyle dedi ben abartmadım ki abartmayı severim, çok ilginç ve komik gelmişti bize 🙂 )
Sonuç olarak aşağıda farklı sınıflamaları ve kullanılan terminolojileri tablo halinde görüyorsunuz.
29 Temmuz 2016 tarihinde Prof. Dr. Süleyman Engin Akhan tarafından yayınlanmış ve 27 Ağustos 2016 tarihinde de son güncelleme yapılmıştır.